Digital Media and Clinical Excellence - The Portsmouth Experience
Digital Media at Portsmouth
The Slides
The Talk
This is based around a talk that I gave at the Royal College of Emergency Medicine in September 2016. The talk focussed on two main areas:
1) How you can use digital media to improve your personal educational experience as helping you as a trainer
2) Using digital media to enhance the reputation of your department by promoting your services, your story, your value and your team
Background
My departments use of social media through twitter, our own departmental website, as well as innovations with the affordable use of other digital media was recognised by the CQC when they inspected our unit in Portsmouth in 2015. We were awarded an ‘outstanding rating’. We have also received a number of plaudits for our work around digital media and innovation.
1) How you can use digital media to improve your personal educational experience as helping you as a trainer
So what I mean is using our current digital age to allow educational resources and information to be available at your finger tips and then being able to share it widely and discuss it with anyone around the globe
This includes:
1. Rapid access to useful articles & engaging in simple discussion using twitter, facebook and reddit
2. Using websites and blogs
3. Creating a repository or personal library using feed aggregators to pull that information and then store it on your phone, ipad, laptop
4. Listening to presentations through podcasts and watching conferences live through videocasts
It can be as simple as recording your departmental teaching so that you then create a library of resources for those trainees that cannot attend or for induction purposes. St. Emlyns have done this for new starters to EM
Lots more on this at ICS State of the Art 2015 Social Media workshop
This all needs to be high quality, have some form of peer review process and ideally free and open access without the need for subscriptions or be hidden behind paywalls
Do we really need this? YES
Lets go back to the 1950’s…
Learning was easy. If you do a pubmed search under ‘intensive care’ or ‘critical care’ there will be 1 article returned.
‘Basically, all that is required is the current issue of The Journal, an easy chair, pencils, a pad of paper and postal cards, along with a genuine, sustaining interest in all fields of medicine’
Do the same literature search for 2015 and there are 24,000 citations. Let’s say only 1 % are relevant, you would still need to read 50 articles every single week to keep up to date. We need to adapt…
1) How you can use digital media to improve your personal educational experience as helping you as a trainer
2) Using digital media to enhance the reputation of your department by promoting your services, your story, your value and your team
Background
My departments use of social media through twitter, our own departmental website, as well as innovations with the affordable use of other digital media was recognised by the CQC when they inspected our unit in Portsmouth in 2015. We were awarded an ‘outstanding rating’. We have also received a number of plaudits for our work around digital media and innovation.
1) How you can use digital media to improve your personal educational experience as helping you as a trainer
So what I mean is using our current digital age to allow educational resources and information to be available at your finger tips and then being able to share it widely and discuss it with anyone around the globe
This includes:
1. Rapid access to useful articles & engaging in simple discussion using twitter, facebook and reddit
2. Using websites and blogs
3. Creating a repository or personal library using feed aggregators to pull that information and then store it on your phone, ipad, laptop
4. Listening to presentations through podcasts and watching conferences live through videocasts
It can be as simple as recording your departmental teaching so that you then create a library of resources for those trainees that cannot attend or for induction purposes. St. Emlyns have done this for new starters to EM
Lots more on this at ICS State of the Art 2015 Social Media workshop
This all needs to be high quality, have some form of peer review process and ideally free and open access without the need for subscriptions or be hidden behind paywalls
Do we really need this? YES
Lets go back to the 1950’s…
Learning was easy. If you do a pubmed search under ‘intensive care’ or ‘critical care’ there will be 1 article returned.
‘Basically, all that is required is the current issue of The Journal, an easy chair, pencils, a pad of paper and postal cards, along with a genuine, sustaining interest in all fields of medicine’
Do the same literature search for 2015 and there are 24,000 citations. Let’s say only 1 % are relevant, you would still need to read 50 articles every single week to keep up to date. We need to adapt…
Shift patterns are changing; learning opportunities are different; individual styles of learning are evolving; web based resources are expanding. We need to stop the cycle of teaching sessions which can end up with lonely trainers and unsatisfied trainees. We need to share the best learning experiences and make them available for all at any time and any place. Digital Media can be used to help us.
Twitter is an incredible way of signposting resources, interacting and networking with similar like minded health care professionals. If you don’t have a twitter account I do encourage you to at least try it. Twitter is really just the start and the way most health care professionals begin to use digital media to enhance their learning.
Websites, blogs and podcasts
Websites offering open access resources and discussion forums allow you to rapidly improve knowledge translation and engage with experts and research investigators. It allows you to keep up to date with the medical literature. Open access resources whether they are websites, podcasts and video-casts mean that you can tap into these resources at time that suits you. Perhaps listen to a podcast whilst in the gym or driving to work? This is the concept of asynchronous learning where individuals may end up learning the same material at different times and locations. It allows trainees to educate themselves in a way that suit their needs at times that suit them.
A comprehensive list of websites, blogs and podcasts can be found at Life in the Fast Lane. Alternatively, you can use google FOAM search
Traditional Teaching
We must not forget the established methods for learning that have served us well for generations. Nothing can and should ever replace this. Learning from an experienced mentor who is able to assimilate knowledge, appraise it and combine it with their wealth of experience is fundamental to the learning process. Social media & specifically FOAM can be used as adjuncts to support this educational experience. Making learning, easily accessible and enjoyable.
2) Using digital media to enhance the reputation of your department by promoting your services, your story, your value and your team
One of the first things I developed when I started as the clinical IT lead was a departmental website. The advantage of having your own departmental website is the freedom that it affords you to show what you offer to the public. It also provides a repository of the incredible work generated from your team. We also have used it as an educational hub with lots of educational resources and induction material for new members of our teams. Examples our work includes: training and induction material; over 40 guidelines; our safety ‘watch out notices’; research opportunities; innovations (such as TiM, BRAD and iSi) and our publications. Please do take a look around our website. Everything is open access.
Our SOP’s and Guidelines - available here
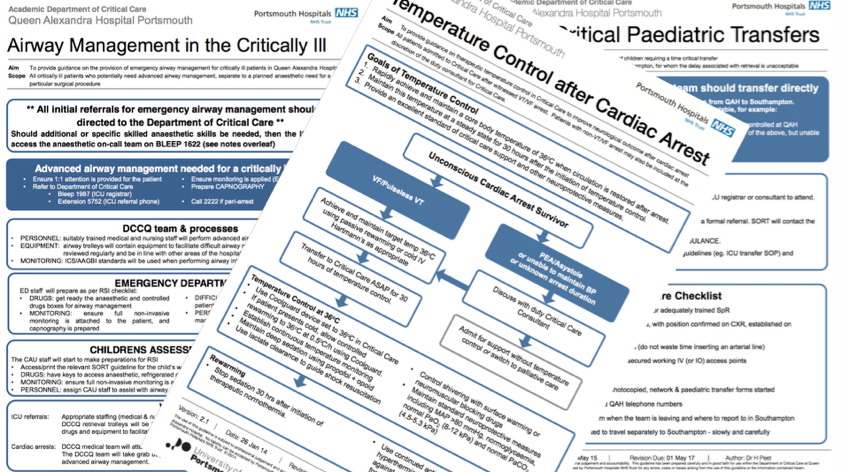
It’s amazing how something as simple as putting some passion and energy into updating guidelines really builds a team spirit. This was an unexpected but welcome finding when we began this project in 2014. Everyone in our department contribute to them and they have become truly multi-disciplinary efforts. We have rebranded them and importantly put them out there for everyone to see and benefit.
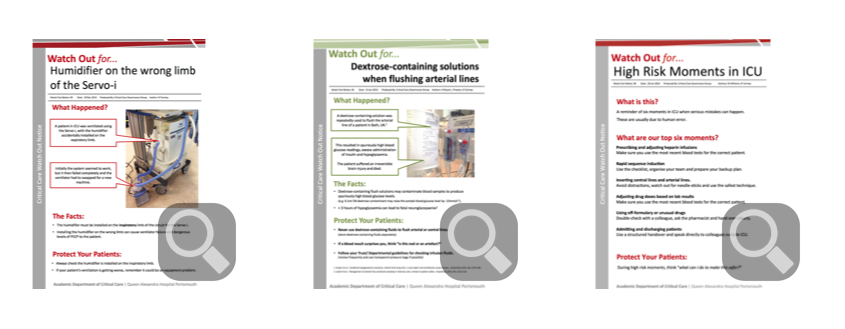
Patient Safety - ‘Watch Out’ notices - available here
We have a growing library of ‘Watch out’ notices which have been created by members of our department. These serve as effective, quick reminders of potential high risk moments in Intensive Care and as a valuable educational resource. Our ‘Watch Out’ notices are displayed electronically on TiM and are rotated throughout the course of a shift. Our TiM screens are located near our blood gas analyser (concept of ‘learning in one minute’ whilst waiting for a sample to be processed) and where we meet to have our daily safety brief.
Meet TiM (The Information Manager)

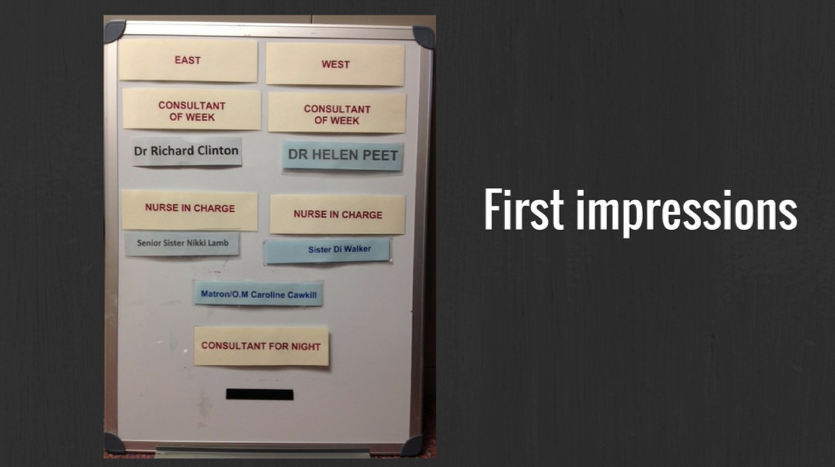
This was our ‘who’s who’ board in 2011. With the use of Raspberry Pi technology, departmental innovation and an effective interface between health care professionals and IT experts, we have initiated an affordable (£ 50 + monitor!) quality improvement project.

Interaction is handled through an input device called a rotary encoder and PIR motion sensor triggers the screen saver during inactivity.
You can set up different templates and uses so we now use this technology for safety screens; patient, relative or staff information and as educational portals
You can set up different templates and uses so we now use this technology for safety screens; patient, relative or staff information and as educational portals
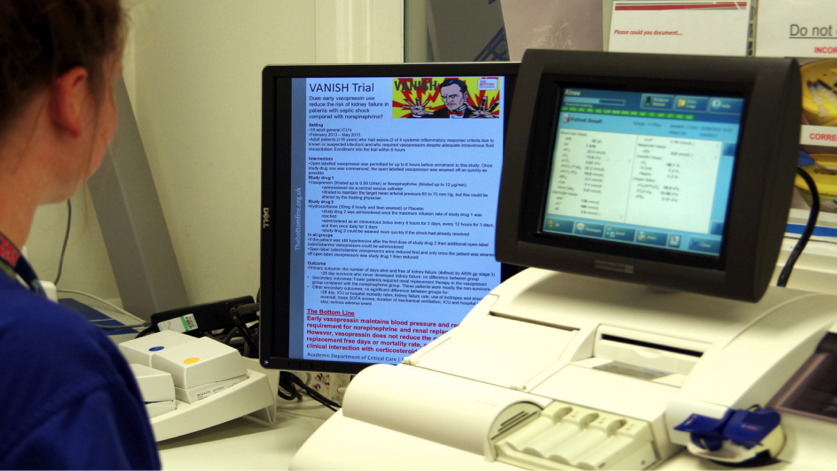
Here is an example of one of our educational hubs. Whilst an arterial blood gas is being analysed (takes about one minute), there is an opportunity to update on the most recent research or patient safety reminders
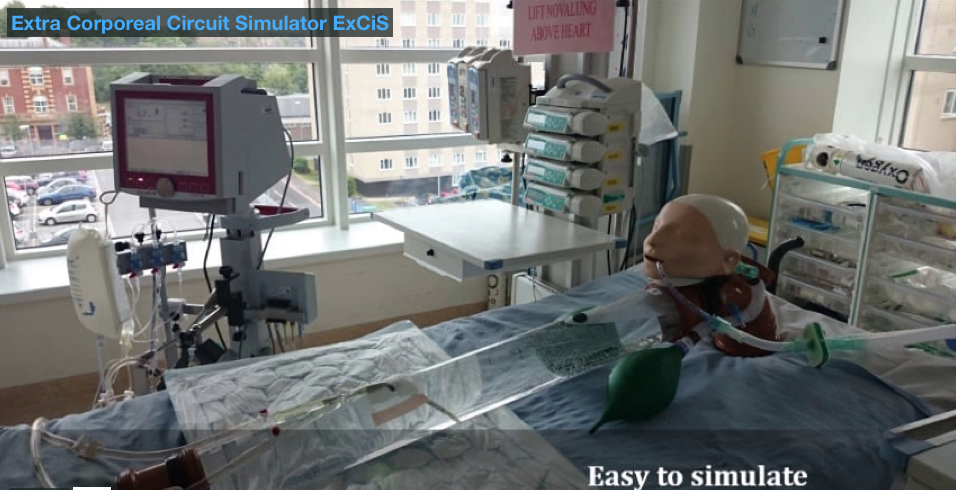
Extra Corporeal Circuit Simulator EXCIS
Extra corporeal circuits are incorporated into many forms of advanced organ support systems e.g. Extra Corporeal Lung Assist (ECLA), Renal Replacement Therapy. An important part of their implementation in any critical care setting is to develop the governance protocols that ensure the patient safety against the potential catastrophic consequences of circuit complications e.g. disconnection.
An inherent component of this is simulation to build team work and mitigate the effect of human factors. There are high definition simulators housed in simulation suites available on the market costing several thousand pounds. These systems are designed and have the capability of delivering a more real-life experience. However, when the issues are related to teaching the mechanics of safe aseptic cannulation, circuit set up, circuit connection and manipulation, simple circuit related troubleshooting and practising circuit complication drills, that level of complexity may not be wanted or required.
When a simulator was required to commission the ILA Activve® extracorporeal circuit purchased to use on patients with respiratory failure in the Critical Department at Queen Alexandra Hospital Dr Kayode Adeniji developed the Extra corporeal circuit sumulator (ExCiS). It represents a cheap alternative to the high fidelity type simulators. It is a re-useable blood volume capacitor that can be repeatedly cannulated and used to demonstrate the setup and running of any kind of extracorporeal circuit (ECMO, ECCO2R, Cardiac Bypass, Renal dialysis, etc.) with components that can be purchased at any local hardware store and put together in your garage.
Though it was designed for simulation on the ilA Activve® ,it can be utilised to model the team-work and procedures needed to manage any extra corporeal circuit and is eminently configurable to the requirements at your institution.
A guidebook and instructional video are available by clicking the image below
An inherent component of this is simulation to build team work and mitigate the effect of human factors. There are high definition simulators housed in simulation suites available on the market costing several thousand pounds. These systems are designed and have the capability of delivering a more real-life experience. However, when the issues are related to teaching the mechanics of safe aseptic cannulation, circuit set up, circuit connection and manipulation, simple circuit related troubleshooting and practising circuit complication drills, that level of complexity may not be wanted or required.
When a simulator was required to commission the ILA Activve® extracorporeal circuit purchased to use on patients with respiratory failure in the Critical Department at Queen Alexandra Hospital Dr Kayode Adeniji developed the Extra corporeal circuit sumulator (ExCiS). It represents a cheap alternative to the high fidelity type simulators. It is a re-useable blood volume capacitor that can be repeatedly cannulated and used to demonstrate the setup and running of any kind of extracorporeal circuit (ECMO, ECCO2R, Cardiac Bypass, Renal dialysis, etc.) with components that can be purchased at any local hardware store and put together in your garage.
Though it was designed for simulation on the ilA Activve® ,it can be utilised to model the team-work and procedures needed to manage any extra corporeal circuit and is eminently configurable to the requirements at your institution.
A guidebook and instructional video are available by clicking the image below
Learning From Excellence

Inspired by the work of Adrian Plunkett and others, we are now trialling electronic favourable event reporting. We believe lessons can be learned from events that have gone well as much as events that might have been done better. We encourage incident reporting and a strong safety culture within our department.
Special thanks go to:
Mike Lympany - IT systems and Development Manager
Nick Tarmey - Guidelines Lead
Kay Adeniji - Developing EXCIS
All members of the Intensive Care Team at Portsmouth
Mike Lympany - IT systems and Development Manager
Nick Tarmey - Guidelines Lead
Kay Adeniji - Developing EXCIS
All members of the Intensive Care Team at Portsmouth